Introduction
Have you noticed a sharp pain on the Discomfort on Outside of Knee of your knee lately? Maybe it started during your morning run, or perhaps it’s been nagging you for weeks while you climb stairs. Either way, you’re probably wondering what’s going on and—more importantly—how to make it stop.
Here’s what most people don’t realize: knee pain on the Discomfort on Outside of the knee is one of the most common complaints physical therapists hear, yet most people try to power through it or ignore it entirely. Big mistake. This type of discomfort usually signals something specific is wrong, and addressing it early can prevent months of frustration down the road.
The good news? Outer knee pain is often fixable without surgery or expensive treatments. In this guide, we’ll walk through everything you need to know about what’s causing your discomfort and exactly what to do about it.
Understanding Outer Knee Pain: What You’re Actually Dealing With

When you say your knee hurts “on the outside,” you’re pointing to one specific area of your knee joint. Understanding the anatomy here helps explain why this particular spot gets injured so often.
The Anatomy of the Outer Knee
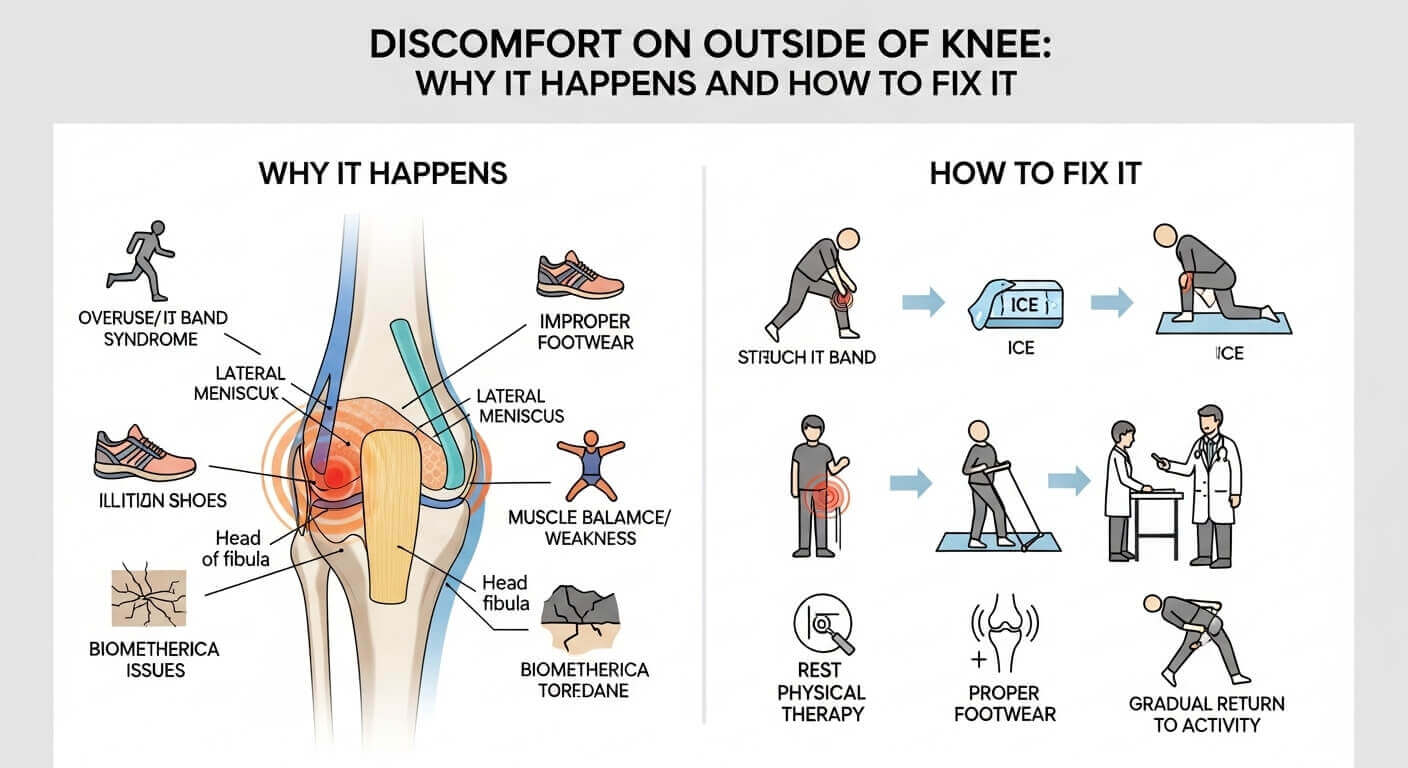
Your knee is a complex joint where three bones meet: your thighbone (femur), shinbone (tibia), and kneecap (patella). But several important structures surround these bones.
On the outside of your knee runs a thick band of tissue called the iliotibial band (IT band). This runs from your hip all the way down to your shinbone. Just below your knee sits the fibular head, where a smaller bone connects to your shin. Between these structures lie cartilage, tendons, and ligaments—all susceptible to injury.
The outside of your knee is basically a network of interconnected parts. When one element gets irritated, inflamed, or injured, it creates that annoying outer knee discomfort you’re experiencing.
Why the Outside of Your Knee Is Vulnerable
The outside knee bears significant stress during movement, especially activities involving repetitive motion or impact. Your IT band and surrounding muscles work overtime to stabilize your knee during running, jumping, and side-to-side movements.
Unlike the inner knee, which has more muscular support, the outer knee relies heavily on the IT band for stability. This makes it particularly vulnerable to overuse injuries.
The Most Common Causes of Outer Knee Discomfort
Let’s identify what’s actually causing your pain. Most cases fall into one of several categories.
IT Band Syndrome: The Runner’s Nemesis
If you’ve been increasing your running mileage recently, there’s a good chance you’re dealing with IT band syndrome. This happens when your IT band becomes tight and irritated, rubbing against the bony prominence on the outside of your knee.
IT band syndrome accounts for approximately 12-15% of all running injuries. It’s the most common cause of outer knee pain in active people. The pain usually feels like a sharp, burning sensation on the outside of your knee that often gets worse when running downhill.
Here’s the tricky part: IT band syndrome doesn’t develop overnight. It’s usually a gradual consequence of muscle imbalances, increased activity, or poor running mechanics. By the time you feel significant pain, the problem has been developing for weeks.
Lateral Meniscus Tears
Your meniscus is a C-shaped piece of cartilage that acts as a shock absorber in your knee. You actually have two—one on the inside (medial) and one on the outside (lateral).
A torn lateral meniscus typically happens suddenly during a twisting motion or change of direction. You might feel a sharp pain, hear a popping sound, or experience sudden swelling. Some people describe it as their knee “giving way.”
Unlike IT band syndrome, which develops gradually, meniscus tears often have a specific moment of injury that you remember clearly.
Lateral Collateral Ligament (LCL) Injury
The LCL is a ligament running along the outside of your knee that provides stability. It prevents your knee from bending inward excessively.
LCL injuries happen from direct contact to the inside of your knee, forcing it outward. You might have experienced this during sports or a fall. Pain from LCL injuries is usually localized right on the outside edge of your knee and worsens when moving side to side.
Knee Cartilage Damage (Chondral Lesions)
The cartilage covering your knee bones can become damaged from repetitive stress, previous injuries, or sudden trauma. Early-stage cartilage damage often causes outer knee discomfort that feels like a grinding or catching sensation.
This is particularly concerning because cartilage doesn’t heal well on its own. Catching early cartilage problems is important to prevent long-term knee degeneration.
Biceps Femoris Tendinopathy
The biceps femoris is a muscle on the back of your thigh that runs down the outside of your knee. When this muscle’s tendon becomes irritated or inflamed, it causes pain on the outer knee, especially below the knee joint.
This often develops from tight hamstrings, weakness in your hip muscles, or overuse from activities like running or cycling.
Peroneal Nerve Irritation
Sometimes outer knee pain actually originates from nerve irritation rather than structural damage. The peroneal nerve runs along the outside of your knee, just below the fibular head.
Nerve irritation causes a different quality of pain—often burning, tingling, or radiating sensations. You might notice numbness in your foot or weakness in your ability to lift your toes.
Red Flags: When You Need Immediate Medical Attention
While most outer knee discomfort isn’t serious, certain warning signs indicate you should see a doctor right away.
Seek immediate attention if you experience:
- Severe sudden swelling that develops within 2-3 hours
- Inability to bear any weight on your leg
- Your knee giving way or buckling
- Signs of infection (redness, warmth, fever)
- Numbness or tingling that extends into your foot
- Severe pain that doesn’t improve with rest and ice
- Visible deformity or your knee looking “out of place”
These could indicate serious injuries like severe ligament tears, meniscus tears requiring surgery, or nerve damage.
How to Diagnose Your Specific Problem
You probably want to know exactly what’s wrong. While only a healthcare provider can officially diagnose your condition, you can gather helpful information about your symptoms.
Questions to Ask Yourself
Start by answering these questions:
When did the pain start?
Gradual onset usually points to overuse injuries like IT band syndrome. Sudden-onset pain suggests acute injury like a ligament tear or meniscus damage.
What does the pain feel like?
Sharp, stabbing pain suggests tendinopathy or ligament injury. Dull, aching pain might indicate muscle strain. Burning pain suggests inflammation or nerve irritation. Catching or grinding sensations point to cartilage issues.
When is it worst?
Pain during specific activities (like running downhill) narrows down the possibilities. IT band syndrome is notorious for hurting during downhill running. Pain when twisting or pivoting suggests meniscus or ligament issues.
What movements make it worse?
This is incredibly valuable information. Pain with direct pressure on the outer knee might indicate a contusion. Pain with side-to-side movements suggests ligament involvement. Pain with weight-bearing or squatting points to cartilage or meniscus issues.
The Physical Examination
You don’t need to be a doctor to perform some basic checks on yourself.
The Noble Compression Test: This simple test can indicate IT band syndrome. Lie on your side with your affected knee bent at a 90-degree angle. Have someone press gently on the outside of your knee. If you feel pain, IT band syndrome might be the culprit.
The McMurray Test for Meniscus Tears: While lying on your back with your knee bent, rotate your shin inward and outward while extending your leg. Pain or a clicking sensation suggests a meniscus tear. Note: This test isn’t 100% accurate, but it’s helpful information for your doctor.
Simple Weight-Bearing Assessment: Stand on your affected leg. Sharp pain with weight-bearing suggests meniscus or cartilage issues. If you can stand pain-free, the problem might be less severe.
Professional Diagnosis: When to See a Doctor
If your discomfort persists beyond two weeks or significantly interferes with daily activities, schedule an appointment with your doctor or a sports medicine specialist.
What to Expect During Your Visit
Your healthcare provider will ask detailed questions about your symptoms, perform physical examination tests, and possibly order imaging. Don’t be surprised if they ask you to demonstrate movements that trigger your pain.
Imaging options typically include:
- X-rays: Show bone structure and can reveal fractures or arthritis
- MRI: Provides detailed images of soft tissue, tendons, ligaments, and cartilage
- Ultrasound: Real-time imaging that’s great for seeing tendon and muscle issues
- CT scan: Sometimes used if MRI isn’t available or you have metal implants
Most mild cases don’t require imaging. Your doctor can often diagnose the issue based on symptoms and physical examination alone.
At-Home Treatment: The First Line of Defense

Before spending money on imaging or expensive treatments, try these initial management strategies. They work for the majority of outer knee pain cases.
The RICE Protocol: Your Starting Point
Rest: Stop doing activities that aggravate your pain. You don’t need complete immobilization—just avoid movements that hurt. If running bothers it, take a running break but walking might be fine.
Ice: Apply ice for 15-20 minutes, four to six times daily during the first 48-72 hours. Use a thin cloth between the ice and your skin to prevent ice burn. Ice reduces inflammation, which is key to pain relief.
Compression: Wrap your knee with an elastic bandage or compression sleeve. This reduces swelling and provides gentle support. Don’t wrap so tightly that you cut off circulation—you should be able to fit a finger under the wrapping.
Elevation: When sitting or lying down, keep your leg elevated above heart level. This helps gravity drain excess fluid from the swollen area.
Most people find significant improvement within 3-5 days of consistent RICE protocol application.
Medications That Help
Over-the-counter anti-inflammatories like ibuprofen (Advil) or naproxen (Aleve) reduce inflammation and pain. Take with food and follow package directions carefully. These work best during the first week when inflammation is highest.
Topical pain relievers like diclofenac gel or menthol rubs provide localized relief without systemic side effects. They’re particularly helpful for IT band pain along the outside of your knee.
Acetaminophen (Tylenol) can ease pain but doesn’t reduce inflammation like NSAIDs do. Use this if NSAIDs upset your stomach.
Progressive Activity Modification
Don’t just stop moving entirely. Instead, modify your activities intelligently.
Week 1-2: Focus on pain-free movement. Walk instead of run. Avoid stairs and hills if they hurt. Perform gentle range-of-motion exercises to maintain flexibility.
Week 2-3: Gradually increase activity as pain decreases. Try swimming or stationary cycling—these often feel better than weight-bearing activities. Walk on flat surfaces before attempting hills.
Week 3+: Return to normal activities gradually. If you were running, alternate run/walk intervals before returning to continuous running.
This progressive approach prevents re-injury while keeping you from losing fitness entirely.
Stretching and Strengthening: The Real Solution
Here’s what separates people who recover fully from those who develop chronic knee problems: targeted exercises.
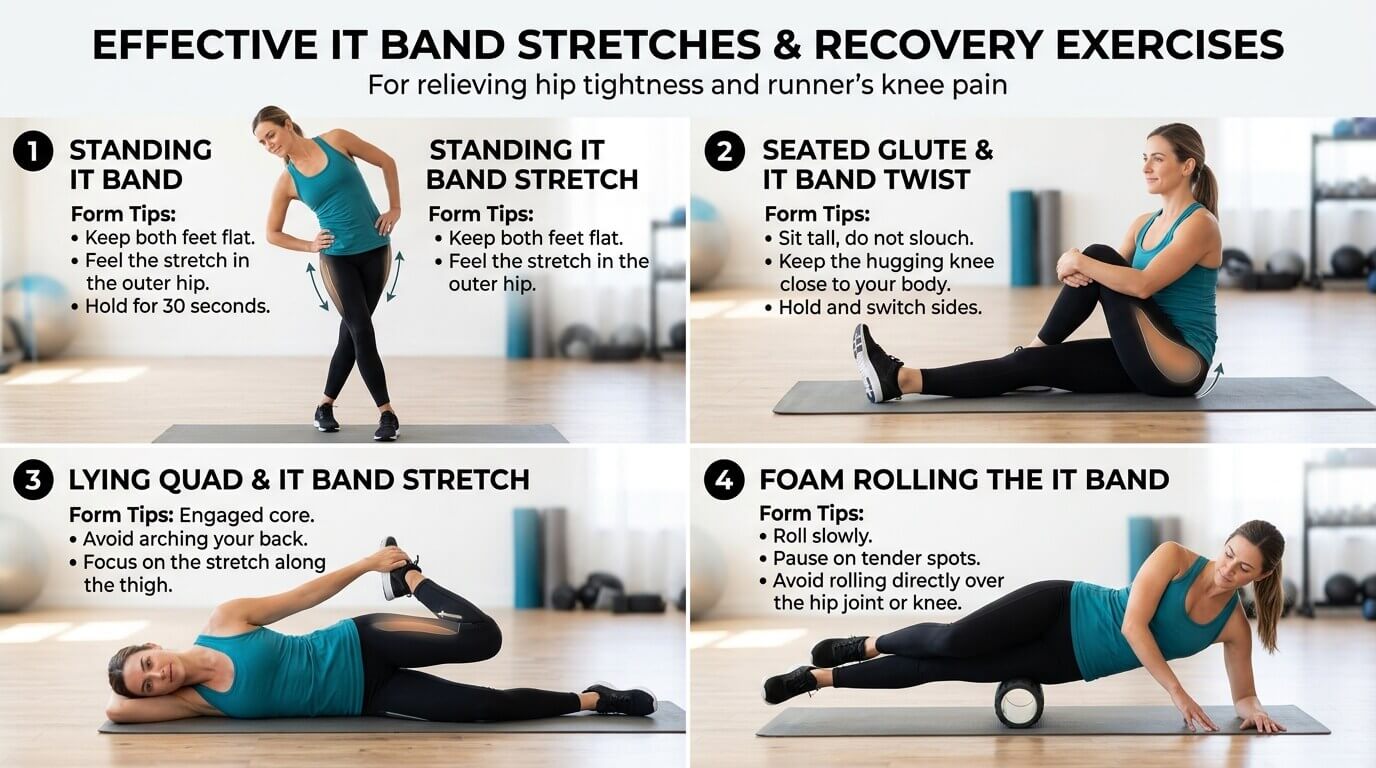
Essential Stretches for Outer Knee Pain
IT Band Stretch: Stand with your affected leg crossed behind your other leg. Lean your hips away from the crossed leg while keeping your spine straight. You should feel a stretch along the outside of your hip and knee. Hold for 30 seconds, repeat 3 times daily.
Piriformis Stretch: Sit in a chair with your affected leg crossed over your other knee. Lean forward gently until you feel a stretch in your buttock. Hold for 30 seconds, repeat 3 times daily. This deep hip muscle greatly influences IT band tension.
Hamstring Stretch: Sit on the ground with one leg extended. Lean forward gently toward your toes. Hold for 30 seconds. Tight hamstrings often contribute to outer knee pain.
Quad Stretch: Stand and pull your foot toward your buttock, keeping your knees aligned. Hold for 30 seconds on each side. This prevents tightness in the front thigh that can contribute to outer knee issues.
Strengthening Exercises That Work
Step-Ups: Use a 6-8 inch step. Step up with your unaffected leg first, then bring your affected leg up. Step down in reverse order. This strengthens the muscles supporting your knee. Start with 2 sets of 10 repetitions.
Clamshells: Lie on your side with knees bent at 45 degrees. Keep your feet together while opening your top knee like a clamshell. This strengthens your gluteus medius, the muscle most commonly weak in IT band syndrome. Do 3 sets of 15 repetitions daily.
Single-Leg Balance: Stand on your affected leg while brushing your teeth or watching TV. This trains proprioception—your body’s sense of where it is in space. Work up to 60 seconds on each side.
Lateral Walks with Resistance Band: Place a resistance band around your legs just above your knees. Walk sideways for 20 steps, keeping slight knee bend and maintaining tension on the band. This directly strengthens the hip muscles stabilizing your knee. Do 3 sets of 20 steps.
Wall Sits: Sit against a wall with your knees bent at 90 degrees, feet flat on the ground. Hold for 20-30 seconds initially, working up to 60 seconds. This builds quad and glute strength. Do 3 sets.
Start with these exercises and progress gradually. If any exercise causes sharp pain (different from the discomfort of working muscles), stop immediately.
Common Mistakes That Make Outer Knee Pain Worse

Most people unconsciously sabotage their recovery. Here’s what to avoid.
Ignoring Your Body’s Warning Signs
Many people experience mild outer knee discomfort and power through it. This almost always makes the problem worse. Pain is your body’s way of saying something isn’t right.
Pushing through pain typically converts minor issues into major ones. If running hurts, take a break from running. If stairs hurt, avoid them temporarily. This isn’t weakness—it’s intelligent self-care.
Stretching Too Aggressively
Some people think more stretching equals faster healing. False. Aggressive stretching of an already irritated IT band can increase inflammation.
Stretch gently and hold for 30 seconds rather than bouncing. If stretching causes sharp pain (not gentle tension), you’re overdoing it.
Neglecting Hip and Glute Strength
This is huge. Many outer knee problems develop because weak hip muscles force your knee to work harder. Skipping hip strengthening exercises means you’re only treating the symptom, not the cause.
Regular hip and glute exercises are non-negotiable for long-term knee health.
Returning to Activities Too Quickly
I understand the temptation. You feel better for a few days, so you return to your normal routine. Then the pain comes roaring back.
Follow the progressive return-to-activity guidelines outlined earlier. Better to return slowly and stay healthy than to rush back and suffer a setback.
Failing to Address Biomechanical Issues
Sometimes, outer knee pain persists because of how you move. Running with improper form, for example, places excessive stress on the IT band.
If pain persists beyond 4-6 weeks despite conservative treatment, consider seeing a physical therapist who can assess your movement patterns.
Physical Therapy: When and Why It Helps
Physical therapy is often the missing piece that transforms people from frustrated and in pain to back to their normal activities.
What a Physical Therapist Does
A good physical therapist doesn’t just give you exercises—they analyze how you move and identify the root cause of your problem. They look at your hip strength, ankle mobility, running form, and movement patterns.
They also teach you proper exercise technique. Doing exercises wrong won’t help and might make things worse. A therapist ensures you’re performing movements correctly.
Typical Physical Therapy Timeline
Weeks 1-2: Assessment, manual therapy (massage and mobilization), and initial exercises focused on reducing pain and improving mobility.
Weeks 2-4: Progression to more challenging strengthening exercises, introduction of balance and proprioception training, and modifications to your daily activities.
Weeks 4-6: Sport-specific or activity-specific training if applicable, introduction of running or sport drills, and preparation for return to full activity.
Most people see significant improvement within 6 weeks of consistent therapy.
Advanced Treatments If Conservative Approaches Fail
If your discomfort hasn’t improved after 6-8 weeks of home treatment and physical therapy, additional interventions might help.
Corticosteroid Injections
Your doctor might recommend an injection directly into the irritated area. This reduces inflammation quickly and can provide significant pain relief. Effects typically last 3-6 months.
Note: Injections are pain management, not a cure. They work best combined with physical therapy and activity modification.
Platelet-Rich Plasma (PRP) Therapy
This newer treatment involves injecting your own concentrated platelets into the injured area. These cells contain growth factors that theoretically promote healing.
Evidence for PRP is mixed, and it’s expensive (usually $500-2000 per injection), but some people report good results, particularly for tendon issues.
Extracorporeal Shockwave Therapy (ESWT)
This treatment uses sound waves to stimulate healing in damaged tissue. Some evidence supports its use for tendon problems like biceps femoris tendinopathy.
Effectiveness varies, and it’s not covered by most insurance plans.
Surgery: The Last Resort
Surgical intervention is rarely needed for outer knee pain. However, if you have a significant meniscus tear causing mechanical symptoms (catching, locking, giving way) or cartilage damage not responding to conservative treatment, surgery might be necessary.
Arthroscopic surgery (minimally invasive) is the typical approach. Recovery usually takes 6-8 weeks.
Prevention: Never Experience This Again
Once you’ve dealt with outer knee pain, you want to prevent it from returning. Here’s your prevention strategy.
The Strength-Maintenance Program
Continue doing hip and glute strengthening exercises indefinitely—even after pain completely resolves. These exercises are your insurance policy against future problems.
Perform clamshells, step-ups, and lateral walks twice weekly as maintenance. This takes just 15 minutes and prevents recurrence.
Smart Training Progression
If you’re an athlete or regular exerciser, follow the 10% rule: never increase activity more than 10% per week. This means distance, intensity, or frequency should increase gradually.
Sudden jumps in mileage or intensity are a recipe for overuse injuries.
Proper Footwear and Equipment
Worn-out shoes contribute to knee stress. Replace running shoes every 300-500 miles. Look for shoes appropriate for your foot type (neutral, stability, or motion control).
If you bike, ensure proper bike fit. Incorrect saddle height and position cause IT band and outer knee stress.
Regular Flexibility Maintenance
Spend 10 minutes daily stretching your hip flexors, IT band, hamstrings, and calves. This maintains the flexibility necessary to prevent muscle imbalances.
Listen to Minor Pain
At the first sign of outer knee discomfort, reduce activities and apply ice. Early intervention prevents minor problems from becoming major ones.
Key Takeaways: Your Outer Knee Pain Action Plan
Outer knee discomfort, while annoying, is typically very treatable. Here’s your roadmap:
Immediate steps (today):
- Rest from aggravating activities
- Apply ice for 15-20 minutes, 4-6 times daily
- Wrap your knee with a compression sleeve
- Take an anti-inflammatory if appropriate
This week:
- Perform the stretches described above daily
- Begin strengthening exercises for hips and glutes
- Assess what activity triggered the pain and modify it
- Avoid hills, stairs, and running if they hurt
If pain persists beyond 2 weeks:
- Schedule an appointment with your doctor or physical therapist
- Continue home exercises and activity modification while awaiting your visit
- Consider over-the-counter pain relief medication
Long-term strategy:
- Commit to hip and glute strengthening exercises indefinitely
- Maintain flexibility through regular stretching
- Progress activities gradually using the 10% rule
- Invest in proper footwear and equipment
Most importantly: don’t ignore outer knee pain or assume it will resolve on its own. Early action prevents chronic problems. With proper treatment, most people return to full activity within 4-8 weeks.
Your knees carry you through life—treat them well, and they’ll reward you with pain-free, active years ahead.