Introduction
Have you noticed a painful, bony bump on the back of your heel that makes wearing your favorite shoes absolute torture? Maybe you’ve started limping after long walks, or perhaps your heel is so tender that even the softest shoe rubs it raw.
If this sounds familiar, you might be dealing with Haglund’s deformity—a condition so commonly triggered by tight shoes that it’s earned the nickname “pump bump.” But here’s what most people don’t realize: this isn’t just about annoying shoe friction. Left untreated, this condition can lead to chronic pain, bursitis, and long-term mobility problems.
The good news? Most cases of Haglund’s deformity respond well to conservative treatment when caught early. In this comprehensive guide, we’ll walk through everything you need to know—from understanding what’s actually happening in your heel to specific treatment strategies that work.
What Is Haglund’s Deformity? Understanding the Anatomy

Before we dive into treatment, let’s get clear on what’s actually going on in your heel. Understanding the condition helps you make smarter decisions about managing it.
The Bony Bump Explained
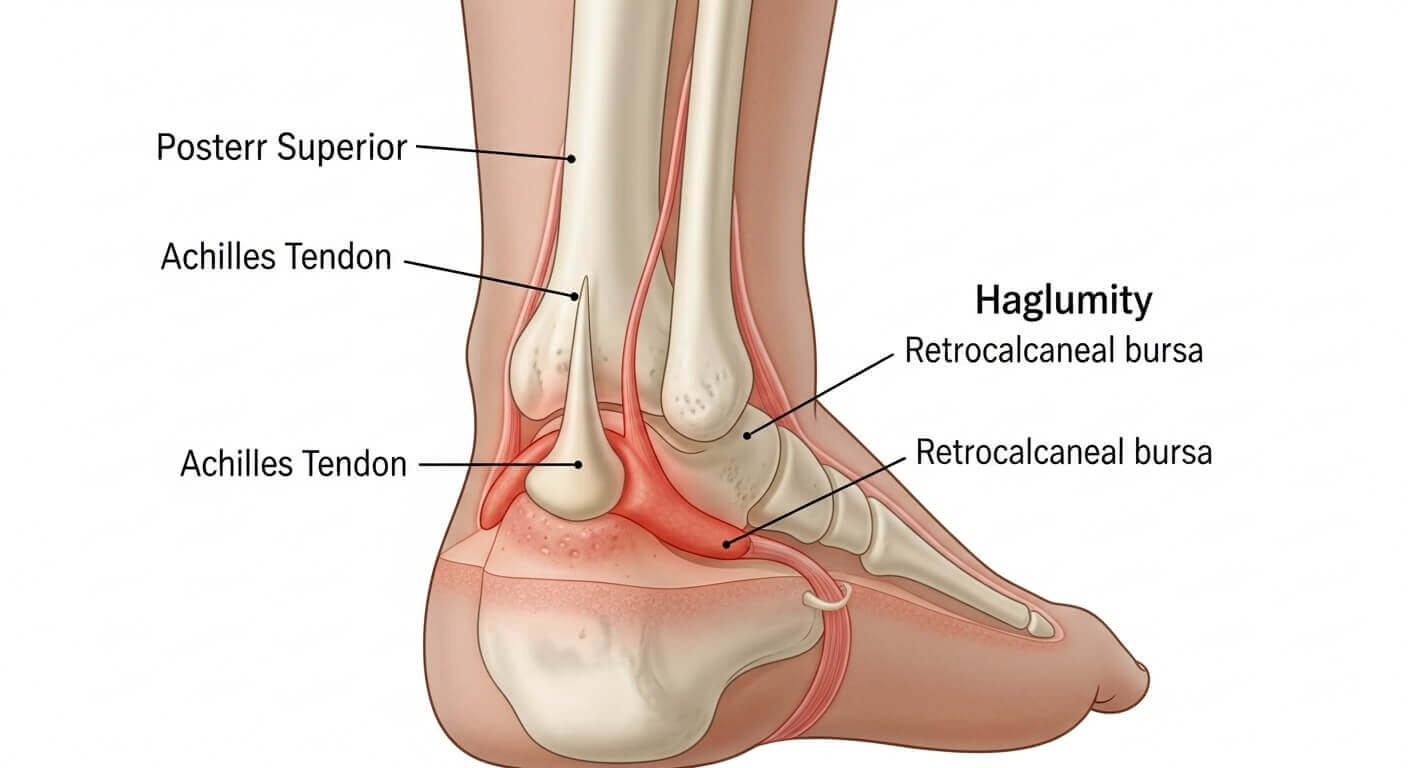
Haglund’s deformity is a bony enlargement on the back of your heel bone (calcaneus), right where your Achilles tendon attaches. This prominent bump sticks out more than normal, creating friction against the back of your shoes.
The bump itself is bone—it’s not swelling or fluid (though those can develop around it). Some people are born with heel bones shaped this way, while others develop the prominence over time due to pressure and biomechanical factors.
Think of it like a speed bump on the back of your heel. Every time your shoe presses against this area, it creates friction, irritation, and inflammation.
The Bursitis Connection
Here’s where things get more complicated. Between your heel bone and Achilles tendon sits a small, fluid-filled sac called the retrocalcaneal bursa. This bursa acts like a cushion, reducing friction between your tendon and bone during movement.
When the bony bump of Haglund’s deformity is present, it constantly irritates this bursa. The bursa responds by becoming inflamed and swollen—a condition called retrocalcaneal bursitis. This is actually what causes most of the pain associated with Haglund’s deformity.
So when doctors talk about “Haglund’s deformity with bursitis,” they’re describing both the underlying bony problem and the soft tissue inflammation it causes.
Who Gets Haglund’s Deformity?
This condition affects both men and women, though women wearing high heels or pumps (hence the “pump bump” nickname) report it more frequently. The typical age of onset is 20-30 years old, though it can develop at any age.
Certain foot structures make you more susceptible:
- High arches (pes cavus)
- Tight Achilles tendons
- A tendency to walk on the outside of your heel
- Naturally prominent heel bone shape (hereditary component)
Athletes, particularly runners and people who do activities involving repetitive heel impact, face a higher risk. Anyone who wears rigid-backed shoes regularly—from work boots to ice skates—also has increased susceptibility.
Recognizing the Symptoms: Is It Really Haglund’s Deformity?
Accurate self-diagnosis helps you seek appropriate treatment. Here’s what to look for.
The Telltale Signs
Visible bump: The most obvious sign is a noticeable bony protrusion on the back of your heel, usually on one or both sides of where your Achilles tendon attaches. When you look at your heel from the side, you’ll see an enlarged, prominent bump.
Pain location: The pain centers right where the bump is, particularly where your shoe counter (the stiff back part) presses against it. The pain typically worsens throughout the day as the shoes continue rubbing the area.
Redness and swelling: The skin over the bump often appears red, inflamed, and may feel warm to the touch. Some people develop a thick, callused area from constant friction.
Achilles tendon pain: Because the inflamed bursa sits right next to your Achilles tendon, you might experience pain along the tendon itself. This can make activities like walking uphill, climbing stairs, or rising on your toes particularly uncomfortable.
How It Differs From Other Heel Conditions
People often confuse Haglund’s deformity with other heel problems. Here’s how to tell the difference:
Achilles tendinitis: Involves pain and inflammation in the Achilles tendon itself, usually 2-4 inches above where it attaches to your heel. The pain is along the tendon, not primarily at the bony bump.
Plantar fasciitis: Causes pain on the bottom of your heel, especially with your first steps in the morning. Haglund’s deformity hurts at the back of your heel.
Heel spurs: Bony growths that form under your heel bone (not behind it). These cause bottom-heel pain similar to plantar fasciitis.
If you have a visible, palpable bump on the back of your heel combined with pain at that specific location, Haglund’s deformity is the likely culprit.
Severity Levels
Mild: Small bump, occasional discomfort with certain shoes, no visible inflammation. This often responds quickly to conservative treatment.
Moderate: Larger bump, consistent pain with most closed-back shoes, visible redness, and swelling. May require several months of treatment.
Severe: Large, prominent bump, constant pain even in soft shoes or barefoot, significant inflammation, thick calluses or blisters. Might need surgical intervention if conservative treatment fails.
Conservative Treatment: What Actually Works
Most people with Haglund’s deformity never need surgery. Here’s your step-by-step conservative treatment plan.
Immediate Pain Relief Strategies
Ice therapy: Apply ice to the painful area for 15-20 minutes, 3-4 times daily, especially after activities that aggravate symptoms. Use a thin towel between the ice and your skin to prevent ice burn.
Create a “heel ice wrap” by filling a plastic bag with ice, wrapping it around your heel, and securing it with an elastic bandage. This provides better coverage than just placing ice against one side.
Anti-inflammatory medication: Over-the-counter NSAIDs like ibuprofen or naproxen reduce both pain and inflammation. Take with food and follow package directions. These work best when taken consistently for 7-10 days, not just when pain is severe.
Elevation: When sitting or lying down, elevate your foot above heart level. This reduces blood flow to the area, decreasing swelling and throbbing pain.
Footwear Modifications: Your Most Important Intervention
Changing what you put on your feet makes the biggest difference in Haglund’s deformity management.
Choose backless or open-heel shoes: Sandals, clogs, or shoes without a heel counter eliminate direct pressure on the bump. Wear these whenever possible during the healing phase.
Look for soft heel counters: When you must wear closed-back shoes, choose ones with soft, flexible heel counters. Athletic shoes designed for running often have padded, flexible heel areas.
Avoid rigid-backed shoes: Stay away from dress shoes, pumps, boots with stiff backs, or any footwear that presses firmly against your heel. Even if you love those shoes, they’re making your condition worse every time you wear them.
Consider heel lifts: Small heel lifts placed inside your shoes (about 1/4 to 1/2 inch) shift pressure away from the prominent bump. This changes the angle at which your heel contacts the shoe, often providing significant relief.
Padding and Protection Techniques
Heel pads and cushions: Gel heel cups or donut-shaped pads with a cutout for the bump can protect the area from shoe friction. Apply these inside your shoes at the heel.
Moleskin or padding: Cut moleskin or adhesive padding to fit around (not on) the bump, creating a buffer zone. This raises the surrounding area slightly, preventing direct pressure on the painful prominence.
Silicone heel sleeves: These slip over your heel like a sock and provide cushioning all around the heel area. Many people find these more comfortable than adhesive pads.
Stretching Exercises: Addressing the Root Cause
Tight Achilles tendons contribute significantly to Haglund’s deformity by pulling on the heel bone and increasing pressure on the bursa. Daily stretching is non-negotiable.
Wall calf stretch:
- Stand facing a wall, hands flat against it at shoulder height
- Step back with the affected leg, keeping it straight
- Bend your front knee while keeping your back heel on the ground
- You should feel a stretch in your calf and Achilles area
- Hold for 30 seconds, repeat 3 times
- Perform 3-4 times daily
Towel stretch:
- Sit with your affected leg extended in front of you
- Loop a towel around the ball of your foot
- Gently pull the towel toward you, keeping your knee straight
- Hold for 30 seconds, repeat 3 times
- Do this first thing in the morning and before bed
Step stretch:
- Stand on a step with just the front half of your foot
- Lower your heel below the step level slowly
- Hold for 30 seconds
- Rise back up
- Repeat 10 times, twice daily
Consistency matters more than intensity. Gentle, regular stretching over weeks delivers better results than aggressive stretching for a few days.
Physical Therapy Interventions
A physical therapist can provide treatments beyond what you can do at home.
Ultrasound therapy: Therapeutic ultrasound delivers deep heat to tissues, promoting blood flow and healing in the inflamed bursa and surrounding areas.
Iontophoresis: This technique uses a mild electrical current to drive anti-inflammatory medication through your skin directly to the affected area.
Manual therapy: Targeted massage and mobilization of your foot, ankle, and Achilles tendon can improve flexibility and reduce tension on the heel.
Strengthening exercises: Your PT will prescribe specific exercises to strengthen your calf muscles, improve ankle stability, and correct biomechanical issues contributing to the problem.
Most people attend PT 1-2 times weekly for 4-6 weeks, with continued home exercises afterward.
Advanced Medical Treatments
When conservative measures don’t provide adequate relief after 3-6 months, medical interventions become necessary.
Corticosteroid Injections
Your doctor might recommend a corticosteroid injection directly into the inflamed bursa. This powerful anti-inflammatory medication can provide significant relief.
What to expect: The injection takes just a few minutes in your doctor’s office. You’ll feel a pinch as the needle enters, then a sensation of pressure as the medication is injected. The area might be sore for 24-48 hours before improvement kicks in.
Effectiveness: Studies show that 60-70% of patients experience good to excellent pain relief after a corticosteroid injection. However, relief may be temporary, lasting 3-6 months.
Important limitations: Injections can only be repeated a limited number of times (usually no more than 3 per year) because steroids can weaken your Achilles tendon and increase rupture risk.
Custom Orthotics
Over-the-counter inserts help some people, but custom orthotics prescribed by a podiatrist address your specific foot mechanics.
These devices:
- Correct abnormal foot positioning
- Reduce excessive motion that contributes to heel irritation
- Redistribute pressure away from the prominent heel area
- Support your arch to reduce Achilles tension
Custom orthotics typically cost $400-800 but can be game-changing for people with underlying biomechanical issues.
Immobilization and Casting
In severe cases, your doctor might recommend a walking boot or cast for 4-6 weeks. This eliminates shoe friction while allowing inflammation to resolve.
While inconvenient, immobilization gives your heel the absolute best environment for healing. Many people who were surgical candidates avoid surgery after a period of immobilization combined with PT.
Surgical Options: When Conservative Treatment Fails

Surgery becomes necessary when you’ve tried conservative treatment for 6-12 months without adequate improvement, and pain significantly affects your quality of life.
What Surgery Involves
Calcaneal osteotomy: The surgeon removes the prominent portion of your heel bone, essentially filing down the bump. This eliminates the bony protrusion causing friction.
Bursectomy: The inflamed bursa is removed entirely. Your body will form scar tissue in its place that serves a similar function but without the chronic inflammation.
Achilles tendon debridement: If your Achilles tendon has damage from chronic inflammation, the surgeon removes damaged tissue and repairs the tendon.
Most procedures combine all three techniques for comprehensive treatment.
Recovery Timeline
Weeks 1-2: You’ll wear a walking boot or cast and keep weight off the foot as much as possible. Expect significant swelling and discomfort managed with pain medication.
Weeks 3-6: Gradually increase weight-bearing in the boot. Begin gentle range-of-motion exercises. Swelling slowly decreases.
Weeks 6-12: Transition out of the boot into supportive athletic shoes. Start physical therapy focusing on strength and flexibility. Most people return to desk jobs by week 6-8.
Months 3-6: Progressively return to normal activities. Athletes can typically resume full training by month 4-6.
Full recovery takes 6-12 months, with continued improvement throughout the first year.
Success Rates
Research indicates that 75-90% of patients report good to excellent outcomes after Haglund’s deformity surgery. Pain typically improves significantly, and most people return to their previous activity levels.
However, surgery carries risks including infection, nerve damage, Achilles tendon complications, and prolonged healing. It should truly be a last resort after exhausting conservative options.
Common Mistakes That Make Haglund’s Deformity Worse
Avoid these pitfalls that sabotage recovery.
Continuing to Wear Problem Shoes
I get it—you love those boots, or your dress code requires certain footwear. But continuing to wear rigid-backed shoes while trying to treat Haglund’s deformity is like taking pain medication while repeatedly hitting your thumb with a hammer.
The shoe friction perpetuates inflammation, preventing healing, no matter what other treatments you try. Footwear modification isn’t optional—it’s the foundation of successful treatment.
Inconsistent Stretching
Doing calf stretches for a few days, then stopping when you feel better, guarantees the problem will return. Tight Achilles tendons remain a problem until you address them with consistent, long-term stretching.
Commit to daily stretching for at least 3-6 months. Many people need to continue regular stretching indefinitely to prevent recurrence.
Ignoring Early Symptoms
Many people notice a small bump and mild discomfort but ignore it for months or years. By the time they seek treatment, they have severe bursitis, a large bony prominence, and sometimes Achilles tendon damage.
Early intervention is far more effective. Address the problem when it’s a minor annoyance, and you’ll avoid it becoming a major medical issue.
Expecting Quick Fixes
Haglund’s deformity develops over months or years. It won’t resolve in two weeks. People who expect rapid results often give up on effective treatments prematurely.
Conservative treatment typically requires 3-6 months of consistent effort. Surgical recovery takes 6-12 months. Set realistic expectations and commit to the timeline.
Self-Diagnosing and Self-Treating Serious Cases
While mild cases often respond well to home treatment, moderate to severe cases need professional evaluation. If you have significant swelling, severe pain, or symptoms lasting more than a month, see a podiatrist or orthopedic specialist.
They can confirm the diagnosis, rule out other conditions, and create an appropriate treatment plan.
Expert Tips for Managing Haglund’s Deformity

Here are lesser-known strategies that experienced podiatrists recommend.
The Shoe Modification Trick
If you absolutely must wear a particular pair of shoes, take them to a cobbler who can:
- Cut out a small section of the heel counter where it contacts the bump
- Stretch the heel area to create more room
- Add padding to cushion the heel
This costs $20-50 and can make problem shoes wearable again.
Night Splints for Faster Healing
Wearing a night splint that keeps your foot in a dorsiflexed position (toes pointed toward your shin) while you sleep maintains Achilles flexibility and reduces morning stiffness.
Many people find that adding a night splint to their treatment regimen speeds improvement significantly.
The Ice Massage Technique
Freeze water in a small paper cup. Peel back the top of the cup to expose the ice, then massage the painful area in small circles for 5-7 minutes.
This provides deep cold penetration and massage simultaneously. Many people find it more effective than traditional ice packs.
Taping for Activity
If you need to stay active during treatment, kinesiology tape applied to support your Achilles tendon and heel can reduce stress on the affected area.
Your physical therapist can teach you proper taping technique, or you can find video tutorials online. This allows continued activity with less pain.
Address Both Feet Even If Only One Hurts
If you have Haglund’s deformity on one foot, you likely have the same bony anatomy on both sides. Implement preventive strategies (stretching, proper footwear, orthotics) for both feet to prevent the problem from developing bilaterally.
The Activity Modification Pyramid
During treatment, think of activities in tiers:
Continue freely: Swimming, cycling, yoga (most poses), upper body workouts
Moderate carefully: Walking (short distances in proper shoes), elliptical training, light hiking on flat terrain
Avoid completely: Running, jumping rope, high-impact aerobics, climbing, sports requiring quick directional changes
This keeps you active without aggravating your condition.
Key Takeaways: Your Haglund’s Deformity Action Plan
Let’s consolidate everything into actionable next steps.
If you suspect Haglund’s deformity:
- Examine your heel for a visible, palpable bony bump at the back
- Note whether pain centers where this bump contacts your shoe
- Schedule an appointment with a podiatrist for an official diagnosis
- Take photos of the area to track changes over time
Immediate actions (today):
- Switch to open-back shoes or those with very soft heel counters
- Apply ice for 15-20 minutes to reduce current inflammation
- Start taking an over-the-counter anti-inflammatory if appropriate
- Remove any shoes from rotation that have rigid, stiff heel backs
This week:
- Begin daily Achilles stretching routine (3-4 times per day)
- Purchase heel pads, moleskin, or silicone sleeves for protection
- Consider heel lifts if you have them available
- Identify and commit to wearing only heel-friendly footwear
This month:
- If symptoms haven’t improved with home treatment, schedule a visit to a podiatrist
- Continue consistent stretching without fail
- Take progress photos to objectively assess improvement
- Consider physical therapy if pain persists
Long-term (3-6 months):
- Maintain a stretching routine even after symptoms improve
- Invest in custom orthotics if biomechanical issues are contributing
- Gradually return to normal activities as pain allows
- Keep heel-friendly shoes in your regular rotation
Red flags requiring immediate medical attention:
- Suddenly, severe heel pain after injury
- Inability to walk or bear weight on the foot
- Signs of infection (fever, increasing redness, warmth)
- Numbness or tingling in the foot
- Visible deformity or change in foot shape
Remember: Haglund’s deformity is frustrating but very treatable. Most people achieve excellent results with conservative care—no surgery needed. The keys are early intervention, consistent stretching, appropriate footwear, and patience with the healing process.
Your feet carry you through life. When one develops a problem like Haglund’s deformity, it deserves the time, attention, and proper treatment necessary to heal completely. Commit to the process, and you’ll be back to pain-free walking before you know it.